Surrogate endpoints are endpoints that are not directly related to the clinical outcome of interest but are used as a substitute for it. They are often used in clinical trials to assess the efficacy of a treatment when the actual clinical outcome may take a long time to observe or may be difficult to measure. For instance, in a trial for a new drug to treat high blood pressure, the surrogate endpoint may be the reduction in blood pressure rather than the actual clinical outcome of interest: reduction in the risk of heart attack, stroke, or death.
There are entire books written on surrogate endpoints, but the following are the main points.
Though the term may be construed as a pejorative, companies often must rely on surrogate endpoints at the phase 2/3 stage of the clinical trial for regulatory purposes. Surrogate endpoints may benefit the population by allowing beneficial drugs to be made availble efficiently; however, there is a risk that the endpoint fails to accurately measure clinically significant outcomes, resulting in a product no different to the control, or worse, a product capable of causing adverse outcomes.
But alas, it is rather intuitive to use surrogate endpoints. If one believes that high blood sugar is the causative agent of diabetes mellitus, then it only makes sense to lower blood sugar, and thus measure it. Likewise, a researcher may measure blood pressure for stroke, bone mineral density for fractures, LDL cholesterol for mycardial infarction, etc. Problem is that some of these surrogates are poor proxies for measuring clinically significant outcomes. When reading the literature, one must evaluate whether the significant outcome follows from the surrogate; there must be a casual connection between the surrogate and the significant outcome.
The question then becomes: how does one establish a causal association between the surrogate and the significant outcome?
A researcher must first eliminate—and the reader must confirm this elimination—variables that may affect the association, namely potential prognostic factors. The JAMA article that I previously referred to1 provides a great example: osteoporosis in post-menopausal women. If measuring bone density as a surrogate, you must eliminate factors such as:
maternal history of hip fracture, previous fractures from any site, poor self-rated health, use of longacting benzodiazepines, impaired visual function, and reduced physical activity
Only then is the association independent, though this is not necessarily the only criterion to meet. You need a RCT in order to prove the association.
We can confidently rely on surrogate end points only when long-term randomized trials have consistently demonstrated that modification of the surrogate is associated with concomitant modifications in the target outcome of interest.
Here’s a good example of the failure of a surrogate:
Trials of angiotensin-converting enzyme inhibitors in heart failure treatment have demonstrated parallel increases in exercise capacity and decreases in mortality, suggesting that clinicians may be able to rely on exercise capacity as a valid surrogate.
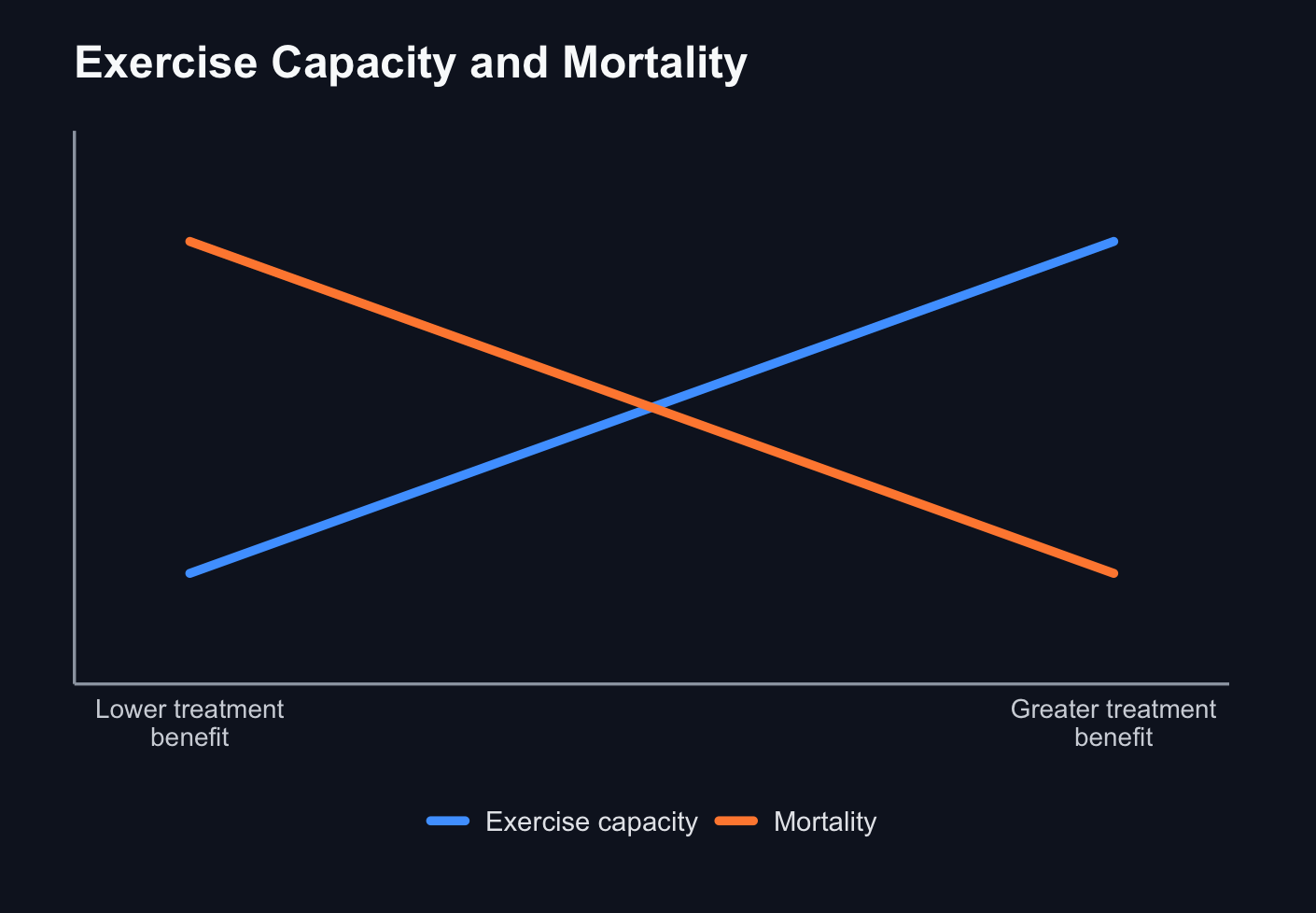
When researchers tried to increase excercise capacity to decrease mortality from heart failure using milrinone and epoprostenol, RCTs showed an increased significant cardiovascular mortality. Here, excercise capacity was a failed surrogate. It’s also important to note how many RCTs show discordant results on the veracity of a surrogate.
Additional posts may follow considering how vast the subject is.
References
Bucher, Heiner C, Gordon H Guyatt, Deborah J Cook, Anne Holbrook, and Finlay A McAlister. n.d. “Users’ Guides to the Medical Literature: Surrogate End Points.” ↩︎